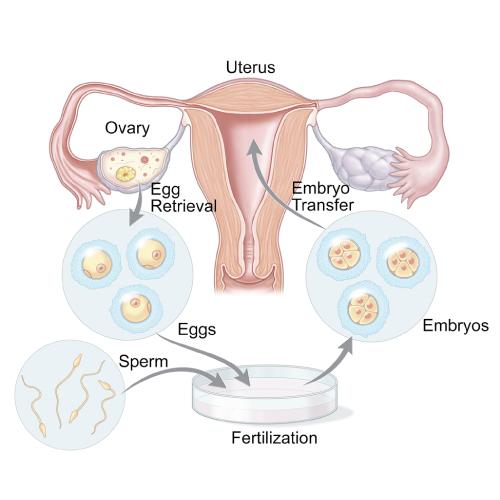
Since the birth of Louise Brown in 1978, the field of ART has grown by leaps and bounds with exciting developments coming to the fore every year, all aimed at making the process safer for the mother. To put it simply, it is a process where we grow an embryo in the IVF lab and then replace it in the uterus.
Though commonly referred to as “test-tube baby”, it does not mean that the baby is actually grown in a test tube in the literal sense!!
This is a 45-minute session which explains in detail all the steps, the success rates, the complications, cost of the cycle, etc.
We use gonadotropin injections to make multiple eggs grow in the ovary, a process called controlled ovarian stimulation. The wife has to come to the clinic at a particular time for daily injections or she can choose to self-administer the injections at home. Starting on day 5 or 6 of starting injection, another medicine called GnRH antagonist will also be added to prevent the eggs from getting released prematurely. So, you will be taking two shots in a day.
This is the name given to an injection which causes the eggs to be released from the follicles. It is given once the follicles reach a certain size, indicating the maturity of the eggs they contain.
This is the procedure by which the eggs are collected from the follicles under ultrasound guidance. It is done under anaesthesia.
This is the step in which the eggs and sperm are joined in the lab, to produce embryos.
IVF – In Vitro Fertilisation – the collected eggs and prepared semen samples are incubated together in a culture dish under controlled conditions.
It can be done in couples where the husband’s sperm counts are normal.
The embryos are allowed to develop over a period of three to five days inside the incubator.
We check for fertilization, i.e., check whether embryo development has started 12-16 hours after fertilization and this is called the “fert check”.
The embryos are allowed to divide further and checked on the day 3 or/and day 5 of culture.
This is the process by which the selected embryos are replaced into the cavity of the uterus in a simple procedure which is almost similar to an IUI.
It is done under ultrasound guidance and does not require any anesthesia in most instances.
This is the 15 day waiting period after embryo transfer when medications and injections may be given on a daily basis to support the growing embryo.
A beta hCG blood test is done at the end of this period to find out the outcome of the IVF cycle.
As we typically replace only a maximum of 2 to 3 day 3 embryos or a maximum of 1 to 2 day 5 embryos at a time, the remaining excess embryos are frozen by a process called vitrification, for future use.
The highly purified recombinant injections used for ovulation induction in an IVF cycle are very expensive by themselves.
The procedure to retrieve the eggs, the process of making the embryos, freezing them and the transfer involves a complex and meticulous combination of drugs, culture media, sophisticated equipment and technical expertise. That is why IVF is more expensive compared to the other treatments
Success rates in an IVF cycle cannot be generalized as they are case-specific and influenced by many factors such as:
Worldwide the success rates are given as 30 to 40 % per cycle. When trying for 2- 3 cycles with cryopreserved embryos, this would then give us a cumulative pregnancy rate of 70 to 80% CDC has designed an IVF success estimator which can help you to roughly predict your chances.
Injections commonly used in an IVF cycle are:
OPU (ovum pickup) or oocyte retrieval is a daycare procedure where the follicles are aspirated transvaginally with ultrasound guidance in the operation theatre, under IV sedation given by an anaesthetist.
The embryologist examines the collected follicular fluid under the microscope and separates the eggs from it. They will inform us about the number of mature oocytes aspirated at the end of the procedure. The retrieved eggs are then placed in the incubator.
It is important to remember that not every follicle may contain an egg and that some may contain immature eggs which are not capable of fertilization.
Hence, the total number of eggs obtained may be lower than the number of follicles documented on ultrasound.
After the procedure, you may need to stay for a few hours till the sedation effect wears off and can then get discharged.
It is a rare condition of unknown reasons where there are no eggs retrieved even after an apparently normal response to ovarian stimulation and a careful aspiration.
Genetic factors, ovarian ageing are some of the reasons known to cause EFS.
OHSS is a potentially serious condition where the ovaries have been overly stimulated by fertility medications. The ovaries may increase in size and produce large amounts of fluid which then leads to pain and bloating of the abdomen.
When there is a strong possibility of OHSS as evidenced by the number of follicles, in PCOS or very high levels of serum estradiol, we may decide to adopt a policy of “Freeze all” and avoid fresh transfer to prevent serious OHSS.
Pre-treatment cycle:
In the cycle or month preceding the intended IVF cycle, we do a set of basic investigations in the male and female partners.
These tests may be omitted in case you happen to have all the relevant reports ready with you (taken within the past 6 months) or may be done in your own country and mailed to us in case you are from out of India.
Yes, you can provide you know or can learn the method of self-administration.
However, the most important consideration is that since the drugs are hormonal preparations they need maintenance at proper cold temperature as per recommendation.
It is very important that they should be maintained properly to ensure the proper efficacy of the drug.
Taking leave during the period of ovulation induction may not be needed unless there is any pain or discomfort caused because of the hyperstimulation of the ovaries.
Since the retrieval of eggs is done under anaesthesia, rest for a day post-procedure may be needed.
Prolonged period of rest is not routinely recommended after embryo transfer also.
Yes, you can. There is no restriction to routine activities as an IVF pregnancy is similar to a natural pregnancy only.
If there are any complications associated with or developed during the course of pregnancy then you may be recommended to avoid certain activities.
An IVF pregnancy is similar to a natural pregnancy in most respects. However, in the first few weeks, extra support of progesterone medications and/or injections may be needed to sustain the growing pregnancy.
There is a slightly increased chance of developing certain pregnancy-related complications like hypertension during pregnancy.
There is no evidence to show an increased risk of birth defects from an IVF pregnancy.
However ongoing studies may answer this question in the future.
IVF cycles have an average success rate of 30-45% per cycle with cumulative pregnancy rates being better.
The major determinant for success is the age of the woman with success rates going down with increasing age.
The quality of embryos (the seed) is another important factor as euploid or chromosomally normal embryos will only result in a live birth.
The endometrial lining and intrauterine environment (the soil) is also a crucial factor as suboptimal environments will lead to decreased implantation and pregnancy rates.
The two-week wait often may seem like the longest and most difficult part of the whole IVF process for many couples.
Spending most of the time wondering whether you will get pregnant or not after putting yourself through so much, is bound to play havoc with our emotions.
One thing you do not have to worry about is whether you’re getting stressed will affect your chances of pregnancy as this association has not been found to be true in studies.
Though IVF may stress you out, YOUR stress is not going to affect your getting pregnant!
Try to keep yourself occupied doing things which relax you or which you love doing, try to get some fresh air every day for some time at least.
For Eg;
At the end of the day, remind yourself that though IVF as a process may fail, that should not be taken as a fact that there is something majorly wrong with you in any manner.
YES, there is a greater incidence of twins or more with assisted reproduction techniques.
But having said that, nowadays with the advent of better technology and knowledge about the risks associated with multiple pregnancies there have been conscious efforts to reduce the incidence of the same.
This is largely by reducing the number of embryos we choose to transfer at one time.
For those who are very particular about avoiding the change of multiple pregnancies, elective single embryo transfer or eSET where we replace only one single blastocyst is an option to consider.
NO, Sex selection is a legal offence in India and is strictly not practiced.